Cannabis and Mental Health
Clients and their families often ask about cannabis use to treat mental health concerns when working with our providers at Navesink Psychological Services in Red Bank, NJ. George Halliwell, LPC often works with clients looking to reduce cannabis use.
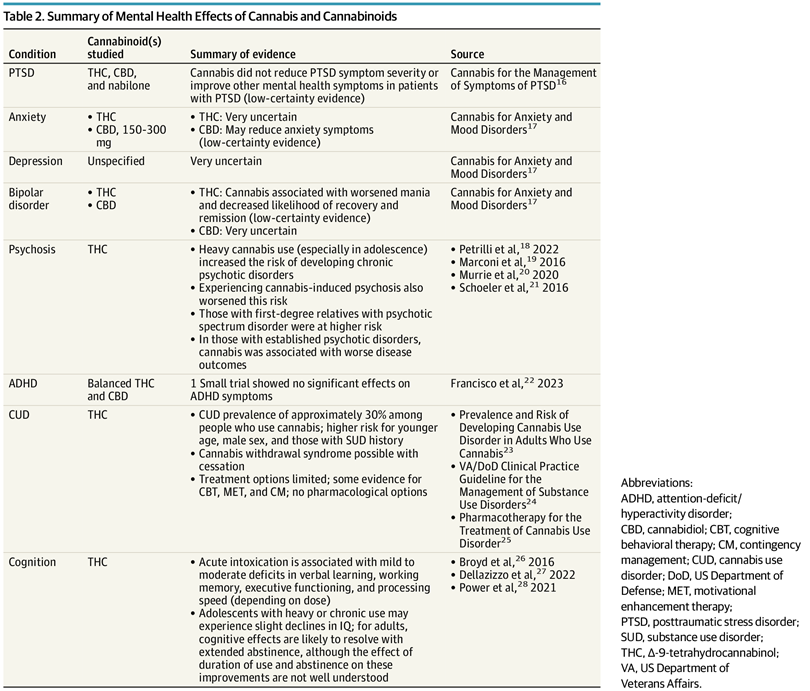
Kansagara, Terry, Ayers, et al. recently published Cannabis and Mental Health A Review describing the current research on cannabis use for mental health conditions as well as the effects of cannabis use. While clients will often report anecdotal evidence that cannabis use improves their mental health conditions, studies have not shown positive effects. Currently, there is no mental health condition for which cannabis is currently supported as a treatment, yet there are substantial documented harms.
Mental Health Diagnoses
For PTSD, Kansagara describe two clinical trials, the largest of which found no difference in PTSD symptom severity between cannabis and placebo. Of note, the sample was 80 veterans so overall the study was small and with a select group of individuals. One small study found nabilone (synthetic THC) reduced nightmares but not sleep quality overall. Evidence is low-certainty and insufficient to recommend cannabis for PTSD.
For Anxiety, THC has unpredictable effects: a low dose (7.5 mg) reduced anxiety in some people, while a higher dose (12.5 mg) induced it. CBD at 150–300 mg/day shows some early promise for generalized and social anxiety disorder, but evidence is still low-certainty and more trials are needed.
For Depression, almost no clinical trials exist. Cannabis does not appear to improve depression, and heavier use is associated with increased suicidality and self-harm.
For Bipolar Disorder, seven observational studies consistently show cannabis worsens mania, reduces recovery, and leads to worse social and employment outcomes. Patients with bipolar disorder should be clearly advised against cannabis use, especially high-THC products.
The area of clearest and most alarming risk is Psychosis. Up to 50% of people who experience cannabis-induced psychosis go on to develop schizophrenia or other chronic psychotic disorders. One 2024 longitudinal study found an 11-fold increased risk of psychotic disorders associated with adolescent cannabis use. Daily use (vs. no use) roughly doubles the risk of psychosis. People with a family history of psychotic disorders are at even greater risk.
Cannabis is frequently self-used for ADHD, but the one small clinical trial found no benefit on attention, memory, or cognition. Acute intoxication actually mimics ADHD symptoms.
About 30% of people who used cannabis in the past year meet criteria for Cannabis Use Disorder (CUD). There are no FDA-approved medications to treat it. Cognitive Behavioral Therapy (CBT), motivational enhancement therapy, and contingency management have some evidence. At Navesink Psychological Services, our team has expertise in CBT, motivational interviewing, and behavioral management, strategies that help clients reduce cannabis use and empower them to make different choices.
In a more general sense, cannabis use impacts Cognition. THC acutely impairs memory, executive function, and processing speed. Adolescents who use regularly may experience lasting IQ declines. In adults, cognitive effects likely improve with sustained abstinence, but the timelines are unclear.
High Risk Groups
While we know that cannabis use does not currently show evidence to treat mental health concerns, it is especially important to consider high risk groups that should be strongly discouraged from cannabis use. These groups include:
Adolescents and young adults (developing brains)
People with bipolar disorder
People with psychotic or psychosis-risk conditions (including those with a first-degree relative with psychosis)
Pregnant individuals (moderate-certainty evidence of preterm birth and low birth weight)
Those with a history of substance use disorder